Leveraging Medicaid Managed Care to Advance Value-Based Payment
By Hailey E. Davis, Senior Manager, Manatt Health | Patricia M. Boozang, Senior Managing Director, Manatt Health
As healthcare costs continue to rise and stakeholders maintain focus on improving quality of care and outcomes, payors for healthcare services are turning to value-based payment (VBP) as one tool to inject greater value into the delivery of care. Medicaid, the nation’s largest health insurer, is no exception. Across the country, state Medicaid agencies are looking to increase provider accountability for cost and quality of care, and many are leveraging their Medicaid managed care programs in new ways toward that end.
Most of the 39 states with comprehensive, risk-based managed care use their contracts with managed care plans to advance payment reforms, increase the proportion of plan payments that are value-based, or enhance the level of risk being assumed by providers.
A Manatt Health review of 39 states’ Medicaid managed care contracts and related sources found that 28 states require plans to engage in VBP with network providers; two other states explicitly encourage or otherwise incentivize plans to engage in VBP. See Figure 1.
Figure 1. VBP Policies in State Medicaid Managed Care Programs
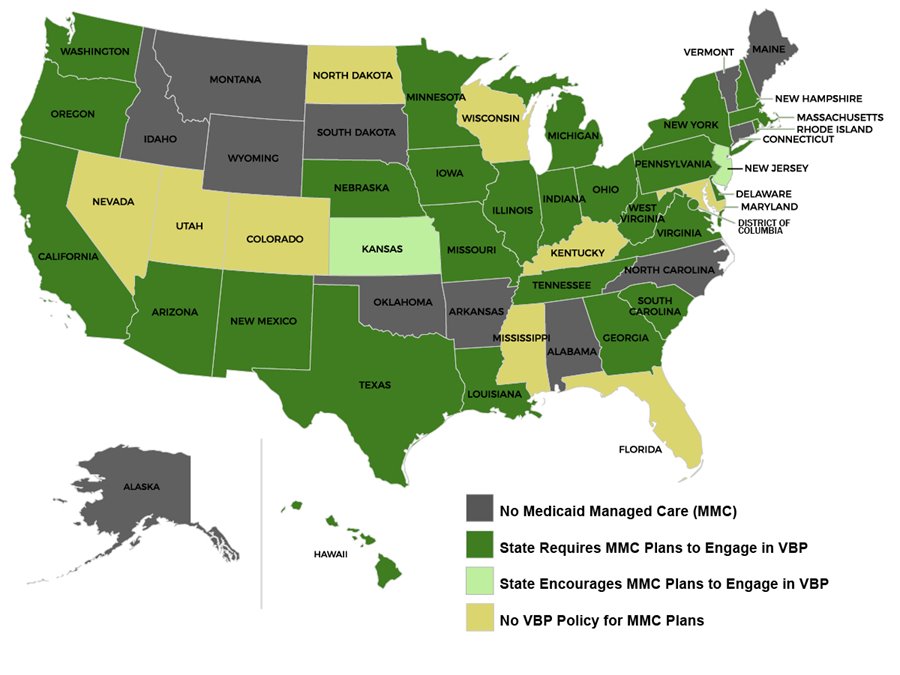
States’ VBP policies can be multifaceted and range from allowing plans to develop and implement their own physician incentive plans to setting minimum thresholds of VBP contracting and conditioning a portion of plans’ capitated premiums on meeting those thresholds:
- 18 states set mandatory VBP targets for plans to meet, either annually or over the course of the contract. Of these states:
- Ten states target a percentage of plan spending or payments to providers made through VBP arrangements;
- Five states target a percentage of members whose care is compensated through VBP arrangements;
- Two states target a percentage of plan contracts that include VBP arrangements; and
- One state, Pennsylvania, targets a percentage of plans’ premium revenue spent in VBP arrangements.
- 13 states financially incentivize plans to engage in VBP. Most of these states have a withhold or incentive program that conditions a portion of plans’ premiums on meeting the state’s VBP requirement(s), such as a VBP target or submission of VBP progress reports. One state, Texas, institutes a per-member-per-month penalty on plans that do not meet the state’s VBP targets. New York State adjusts plans’ rates, both upward and downward, based on the amount and type of VBP contracting and contract performance on cost and quality.
- 12 states require plans to develop and implement a VBP strategy. States are requiring plans to describe their strategies for meeting state VBP targets, increasing VBP over time, ensuring providers are prepared for and incentivized to participate in VBP, and/or directing consumers to providers who participate in VBP or perform well on quality and cost measures. These states generally require plans to submit VBP strategies on an annual basis and report on their progress achieving milestones outlined in the strategies.
- 10 states require plans to participate in state-directed payment reform programs. In some cases, states are requiring plans to implement state-developed episode-based payment models with providers, enter into VBP arrangements with patient-centered medical homes or Accountable Care Organizations (ACOs), and participate in a gain-sharing pilot program.
- 8 states use the Health Care Payment Learning and Action Network (HCP LAN) Alternative Payment Model (APM) Framework in their VBP requirements. These states generally use the APM framework to define levels and types of VBP that plans must pursue.1 Washington State, for instance, sets its multiple VBP targets based on the VBP categories described in the APM framework.
- Some states are making nascent efforts to drive provider VBP implementation through plans. Federal regulations allow plans to develop and implement their own “physician incentive plans,” or “PIPs,” which can include use of VBP models.2 Most states' contracts reference these federal PIP regulations, and several supplement them with their own PIP requirements. Three states—Indiana, Iowa and Missouri—require plans to develop and implement PIPs as part of their VBP policies.
- States are using myriad other tactics to advance VBP. Georgia requires its plans to collaborate with the state on building and implementing its VBP program through participation in the state-established “VBP Performance Management Team.” New Mexico allows plans that do not meet its VBP targets to reinvest funds that would otherwise be taken from them in the form of penalties, so long as the reinvestment is on activities that improve plan systems or directly benefit members. In Texas, plans must dedicate resources to evaluate the impact of VBP arrangements on utilization, quality and cost, as well as return on investment.
Conclusion
In the context of tightening Medicaid budgets and the drive to improve health outcomes, states are expanding VBP in Medicaid and leveraging their Medicaid managed care programs to advance their payment reform goals. VBP policies vary across the country but the trends are clear: states are engaging their managed care contractors in VBP on multiple fronts, increasingly mandating plan action on VBP and providing financial incentives and imposing penalties tied to specific VBP goals. As implementation progresses and results are evaluated, states will hone their approaches to VBP. Essential to continued progress will be collaboration among state policymakers, plans, providers and other stakeholders to develop and implement effective VBP models in Medicaid that align with other major payors’ VBP initiatives.
NOTE:
This analysis was conducted for Insights@ManattHealth, a subscription service that provides a searchable archive of all of Manatt Health’s content and features premium content that is available only to subscribers. In addition to access to state VBP profiles and each state’s Medicaid managed care VBP policies, subscribers have access to: other 50-state surveys; weekly updates of key federal and state health policy activity; detailed summaries of federal Medicaid, Medicare and Marketplace federal regulatory and sub-regulatory guidance; and much more. If you are interested in learning more, please contact Patricia Boozang at PBoozang@manatt.com.
1There are several other states, such as New Mexico and New York, that do not use the APM framework but instead define their own “levels” of VBP.
242 C.F.R. § 438.3(i).
back to top
New Webinar: Redefining Care Management in Medicaid Managed Care
Join us on May 24 from 3:00 to 4:00 p.m. ET and learn how states and MCOs are redefining care management.
States are becoming increasingly demanding in their expectations of managed care organizations (MCOs) when it comes to care management. Formerly a domain solely left to MCOs, many states are pushing health plans to move beyond a cubicle-and-telephonic approach, requiring new care management models that have the potential to change the way care is delivered. What does this mean for MCOs, providers and patients? How have these new requirements been reflected in state contracts with MCOs? What opportunities and challenges does this create for both small practices and provider-led organizations, such as Accountable Care Organizations and Clinically Integrated Networks?
Find out in a new Manatt webinar, “Redefining Care Management in Medicaid Managed Care.” The first program in our new series on Medicaid managed care trends, the session will share new perspectives and developments reshaping the market. Key topics include:
- An overview of evolving care management standards for MCOs across states
- Shifting state, plan and provider expectations around accountability, particularly for high-risk populations
- A discussion of how providers can position themselves to take on new care management opportunities—what’s in it for them, and what the risks are
- Observations for the future, including the blurring of roles, states’ evolving view of where care management functions should be performed, and opportunities arising for all entities to rethink their roles and develop new models
Even if you can’t make our live program on May 24, please click here to register free now, and we will send you a link to view the webinar on demand. And watch for the remaining sessions of our Medicaid managed care trends series throughout the spring, including new programs on children with special healthcare needs and plan enforcement/program compliance.
Presenters:
Benjamin K. Chu, MD, Managing Director, Manatt Health
Melinda Dutton, Partner, Manatt Health
Sharon Woda, Managing Director, Manatt Health
Edith Coakley Stowe, Senior Manager, Manatt Health
back to top